Blog/News
Latest News
BOOST PHYSIO regularly write articles about injuries and conditions. You can search through our database of articles by using the search bar.
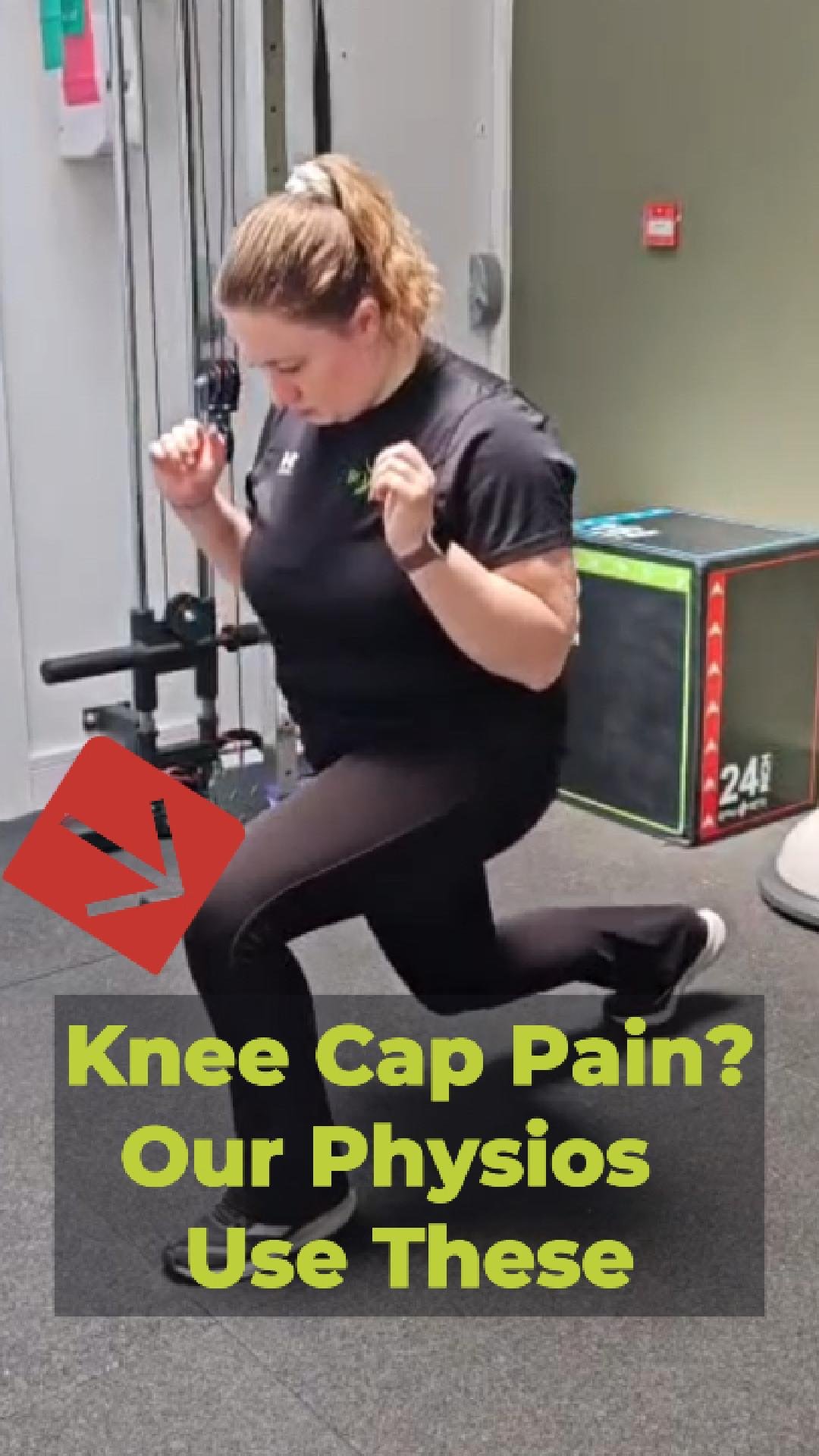
Knee Cap Pain? What is it and how to help it
Does the front of your knee ache when you climb stairs, squat down or sit for long periods? You [...]

Upper Back Physio Stretches
How to Relieve Upper Back & Neck Pain / Stiffness Simple Moves for Desk Workers, Drivers and Anyone [...]

Tennis Elbow Physio Exercises To Help
Tennis Elbow: Why Rest Alone Won't Fix It And the counter-intuitive science that explains why loading your tendon is [...]
Morning Low Back Stretch Routine
Wake Up Your Back: 3 Morning Stretches Your Spine Will Thank You For If your back feels stiff, achy [...]

What Is Causing My Shoulder Pain?
Stiff knee after Total Knee Replacement surgery? One of our physios working to help a patient with a stiff knee bend their knee better.

Do I have a Frozen Shoulder or a Rotator Cuff problem?
Stiff knee after Total Knee Replacement surgery? One of our physios working to help a patient with a stiff knee bend their knee better.

Marathon Runners: Get Race-Ready Promo
Stiff knee after Total Knee Replacement surgery? One of our physios working to help a patient with a stiff knee bend their knee better.
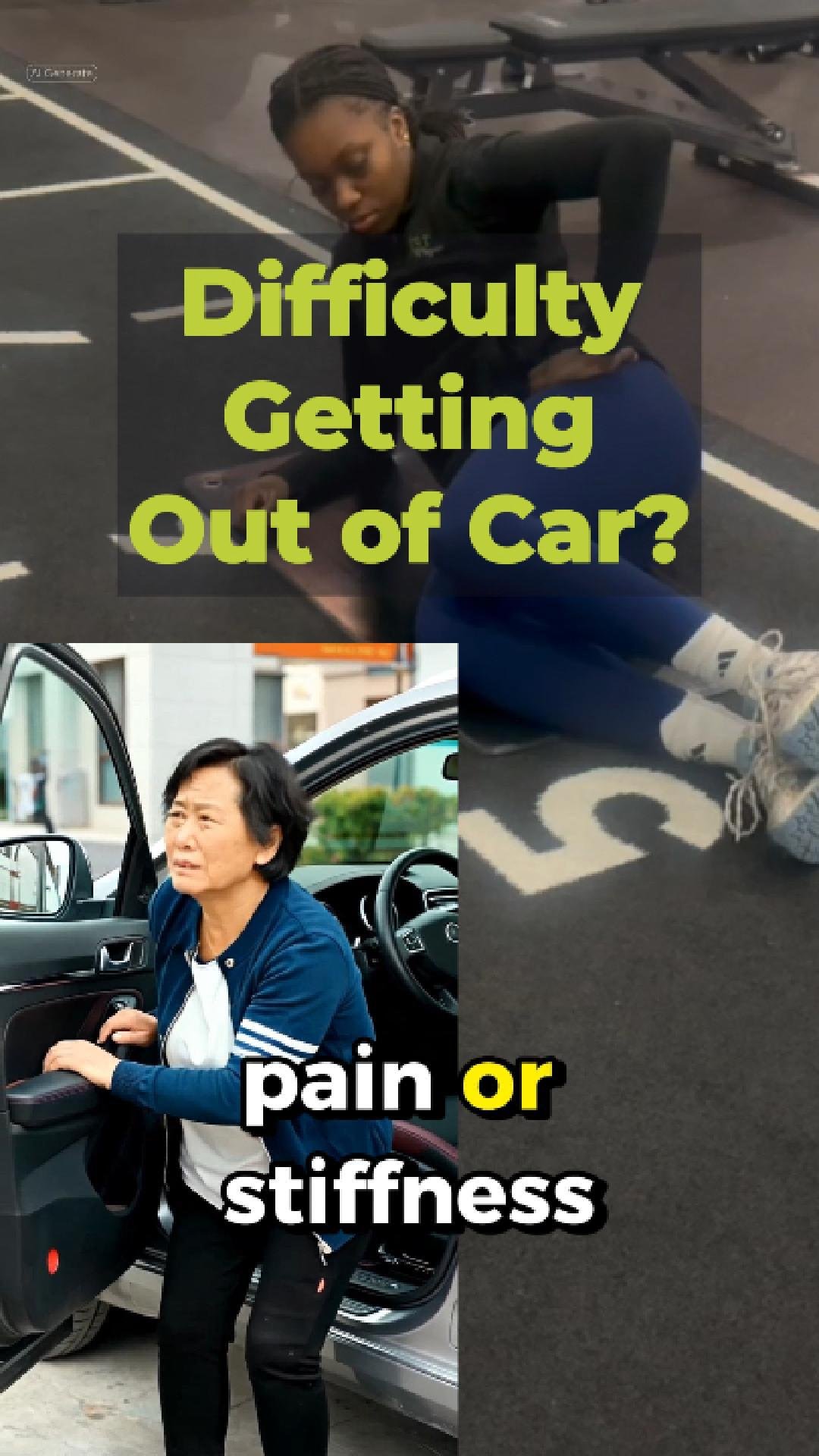
How to make getting out the car easier
Stiff knee after Total Knee Replacement surgery? One of our physios working to help a patient with a stiff knee bend their knee better.

What is a frozen shoulder? Why is early intervention is essential?
Frozen Shoulder- Why early intervention is essential Frozen Shoulder, medically known as Adhesive Capsulitis, is a painful and often frustrating condition that our physiotherapists help people with daily. Frozen shoulder affects movement and everyday function and causes significant pain.












